



More on ICSI
ICSI is successfully performed worldwide since 1992 and it is the most powerful micromanipulation procedure yet with which almost all male infertility factors are treated.
 The therapeutic possibilities of ICSI have made it possible for men with severe sperm defects (low concentration, low motility and poor morphology or ejaculation disorders) to become fathers. In the past, these men would have no hope of experiencing fatherhood.
The therapeutic possibilities of ICSI have made it possible for men with severe sperm defects (low concentration, low motility and poor morphology or ejaculation disorders) to become fathers. In the past, these men would have no hope of experiencing fatherhood.
Practically, a single motile spermatozoon is needed per mature oocyte.
Until today, thousands of babies have been born from ICSI. There is no evidence that micromanipulation affects embryo quality or children’s safety and wellbeing.
Apart from fertilization, the rest of the procedure remains the same as in conventional IVF for the couple.
When is ICSI recommended?
ICSI is used to mainly overcome male factor infertility with abnormal semen parameters. Indications for ICSI are:
→ Severe oligoasthenozoospermia (the cut-off limit in regards to concentration, motility and morphology varies according to several studies).
→ Total absence of motile spermatozoa (azoospermia).
→ Round-headed spermatozoa lacking an acrosome (a rare disorder named globozoospermia).
→ Extensive sperm agglutination.
→ Previous fertilization failure with a phenomenic normal sperm.
Moreover, ICSI is used to treat special cases such as low number or poor quality oocytes, especially in women of advanced age.
ICSI – How is it performed?
 After sperm collection, depending on spermatozoa concentration and motility, the sample is processed, with minor modifications.
After sperm collection, depending on spermatozoa concentration and motility, the sample is processed, with minor modifications.
If the first sperm sample is not adequate, the husband is requested to produce a second sample after a while.
If a few dozens of motile spermatozoa are identified, then ICSI can be performed properly.
If no motile spermatozoa are detected or in the case of obstructive azoospermia spermatozoa are retrieved microsurgically by the epididymis or the testes. (MESA, FNA, TESE).
ICSI is performed in two phases, after egg retrieval.
First, the oocytes need to be exposed to a specialized treatment with an enzyme (hyaluronidase), to remove the cumulus corona cells that surround zona pellucida. This is a crucial manipulation because cumulus corona cells will not be penetrated by spermatozoa, as it occurs in conventional IVF, and this will obstruct clear observation of the oocyte during micromanipulation. When cumulus corona cells are completely removed, oocyte maturation and integrity are assessed. Oocyte maturation is confirmed when the first polar body is present. ICSI can be performed only in mature oocytes, where the first polar body is observed. Immature oocytes cannot be used for treatment.
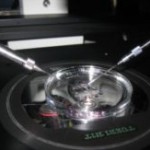
The second phase involves microinjections. Denuded oocytes are placed in plastic Petri dishes, in small drops of culture medium each one. Oocytes are immobilized using a micromanipulator and a thin glass pipette, in a specially equipped microscope. Another thinner glass pipette (injection-like pipette) is used to collect and inject a single spermatozoon in each oocyte. The injection pipette that contains the spermatozoon penetrates the zona pellucida and breaks the cytoplasmic membrane of the oocyte. After injecting the spermatozoon the latter will be maintained in the oocyte cytoplasm. Each injection lasts a few seconds. However, the overall procedure may last many hours, especially if spermatozoa are rare and difficult to identify.
What happens after ICSI?
After injection, the oocytes are placed into the incubator, under stable culture conditions.  Polyspermy is impossible to occur when using ICSI since fertilization is totally controlled by inserting a single spermatozoon into the oocyte. The fertilization rate is usually high (around 75%).
Polyspermy is impossible to occur when using ICSI since fertilization is totally controlled by inserting a single spermatozoon into the oocyte. The fertilization rate is usually high (around 75%).
Complete fertilization failure after ICSI is very unusual and in most cases is probably due to incomplete decondensation of the spermatozoon or failed oocyte activation (e.g. oocytes from women of advanced age).
Oocyte damage during injection is very rare (less than 2-3% in experienced hands). Oocytes that have tolerated the injection have a normal shape (their shape is checked a few minutes after completing the injections and if any oocyte has been damaged, it is removed from culture). Thereafter, the procedure remains exactly the same as in conventional IVF (pronuclei – zygote stage, cleavage in 2, 4, 8, e.t.c. blastomeres, embryo selection and transfer.





